37 YEAR OLD CKD MALE PATIENT WITH FEVER AND SOB
SNEHA CHAUHAN
ROLL NO- 126
2017 BATCH
9th SEMESTER
- This is an online E-log to discuss our patient’s de-identified health data shared after taking his/her/guardian’s informed consent.
- Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
- This E-log also reflects my patient centered online learning portfolio and your valuable inputs on comment box are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competence in reading and comprehending clinical data including history, clinical findings and come up with diagnosis and treatment plan.
Following is the view of my case-
Chief complaints-
Patient came with chief complaints of-
- Fever- since 15 days
- Shortness of Breath- since 15 days.
History of Presenting Illness-
Patient was apparently asymptomatic 15 days ago, then he developed
- Fever-
- Insidious in onset
- Gradual in progression
- Since 15 days
- Of low grade type,
- Relieved on taking medication.
- No other associated symptoms.
- And Shortness of breath-
- Sudden in onset
- Gradually progressing
- Since 15 days
- Relieved on hemodialysis.
Negative History-
No history of chest pain, palpitations, excessive sweating, decreased ruins output, and pedal edema.
Past History-
- There were complaints of pedal edema and facial puffiness in the past, about 5 years ago which were treated accordingly.
- No other similar complaints in the past
- Has history of hypertension since 15 days.
- No history of Diabetes, CAD, Asthma, etc.
Family History-
Family history is Insignificant
Treatment history-
- Tab NICARDIA 20mg OD
- Tab ARKAMINE 0.1mg BD
Personal history-
- Appetite- normal
- Diet- Mixed
- Bowel and Bladder- Regular
- Sleep- adequate
- Habits- Occasionally consumes alcohol.
General physical examination-
Vitals-
- Heart Rate- 78 beats per minute.
- Temperature- Afebrile
- Respiratory rate- 16 cycles per minute
- Blood pressure- 130/80 mmHg
Pallor and Oedema- present


No signs of Icterus, Cyanosis, Clubbing, Lymphadenopathy
Systemic examination-
- Cardiovascular system- S1S2 heard
- Respiratory system-
- Dyspnoea present
- No wheeze
- Centrally positioned trachea
- Vesicular breath sounds
- Abdomen-
- Shape of abdomen- Scaphoid
- Tenderness- not present
- Palpable mass- Not present
- Hernial orifices- Normal
- Free fluid- absent
- Liver- not palpable
- Spleen- not palpable
- Bowel sounds heard
- Central Nervous System-
- Patient was conscious, coherent and alert, with normal speech.
- No signs of meningeal irritation
- Sensory, motor system, reflexes and cranial nerve findings are normal.
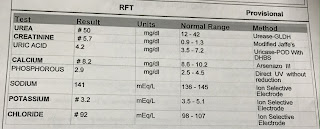
Investigations-







Treatment given :
- Fluid restriction less than 1.5 L/day
- Salt restriction less than 2g/day
- Tab LASIX 40mg PO/BD
- Tab NICARDIA 20mg PO/BD
- Tab NODOSIS 500mg PO/BD
- Tab OROFER PO/BD
- Tab SHELCAL 500mg PO/BD
- Inj ERYTHROPOIETIN S/C once weekly
- Inj HAI S/C according to GRBS
- Tab EPTOIN 100mg PO/TID
- Tab DOLO 650mh PO/BD